kaiser permanente appeal form
The appeals process is available for a member to seek. Kaiser Permanente of Colorado Provider Appeals PO.

Kaiser Permanente Southern California Kpsc 1 Ncpdp Data Elements Version D 0
Appeals for non-coverage Appointment of Representative Authorization to Release PDF Appointment of Representative for Medicare Members PDF Member Appeal Request PDF.
. Kaiser Permanente Medicare Appeals Coordinator PO. Download our appeals policy for members which outlines the appeals process and provides contact information. For further information on fully-funded appeals please refer to the Fully.
If you have questions about this form call the Member Services Call Center at 1-800-464-4000 TTY 1. Appeal is submitted without Appeal Filing Form the. Copy of faxed referral with the.
Kaiser Foundation Health Plan Inc in Northern and Southern California and Hawaii Kaiser. Reason for denial member name medical record number service dates and. Patient Date of Birth.
Fill in the empty fields. Appeals procedures for members in the Hawaii region. If coordination of benefits is involved the provider has 30 months.
Original Claim Amount Paid. Kaiser Permanente Provider Appeals Provider Contracting and Relations 500 NE Multnomah Blvd Ste 100 Portland OR 97232 503-813-3376 503-813-2017 Fax Please note that all claim. Kaiser Permanente Claim ID Number.
Appeals procedures for members in the Mid-Atlantic States region. Get the Kaiser Permanente Appeal Form you need. Box 372970 Denver CO 80237 PROVIDER- CARRIER DISPUTEAPPEAL FORM Please complete the following.
Kaiser Foundation Health Plan of Washington Member Appeals PO. If a provider wishes to appeal on behalf of the member a Statement of Authorized Representative SAR form must also be submitted. Copy of faxed referral with the.
Kaiser Permanente health plans around the country. Non-contracted providers have 60 days from the notification date of denialand will follow the member appeals process. The SAR must be completed and signed by the patient or.
Return completed form to. Copy of the original claim form CMS 1500 or UB04 Copy of the Kaiser denial Other appropriate supporting documentation for referral and timely filing disputes. GRIEVANCEAPPEAL FORM Medicare California By mail to Kaiser Foundation Health Plan.
See What Its Like To Be A Member. Claims disputes Member appeals. Get the Kaiser Permanente Appeal Form you need.
Box 34593 Seattle WA 98124-1593 Online Alternatively you can fill out a form online but to protect the security of. Please send your completed grievance form to the applicable facility or location below. A Healthier Tomorrow Starts With Kaiser Permanente.
Find forms for health services billing and claims referrals and clinical review behavioral health services provider information and more. How to appeal claims as a provider. Kaiser Foundation Health Plan Inc in Northern and Southern California and Hawaii Kaiser Foundation Health.
Original Claim Amount Billed. Patient Date of Birth. Kaiser Permanente health plans around the country.
You may file your GrievanceAppeal by one of the following ways. Kaiser Foundation Health Plan of the Northwest Member Relations Department 500 NE Multnomah St Ste. Involved parties names addresses and phone numbers etc.
Please send your completed grievance form to the applicable facility or location below. Ad Our Doctors Are Dedicated To Providing You High-Quality Comprehensive Care. Use this form to send an appeal to Kaiser Permanente Washington.
100 Portland OR 97232 Fax 1-855-347-7239. Box 34593 Seattle WA 98124-1593 What is a Member Appeal. Kaiser Permanente Medical Record Number.
Open it up with cloud-based editor and start adjusting. Copy of the original claim form HCFA 1500 or UB92 Copy of Kaiser denial Other appropriate supporting documentation for referral and timely filing disputes. If you have questions about this form call the Member Services Call Center at 1-800-464-4000 TTY 1.
Appeal is submitted without Appeal Filing Form the information listed below must be present. If you are submitting this request on behalf of the member you must complete and return to Kaiser Permanente Member Appeals a copy of the following forms.
Kaiser Medical Records Fax Number Fill Online Printable Fillable Blank Pdffiller
Fillable Online Mydoctor Kaiserpermanente Kaiser Permanente Authorization For Use Or Disclosure Form Fax Email Print Pdffiller
Application Kaiser Permanente California
2
Kaiser Permanente Combined Disclosure Form At Your Service
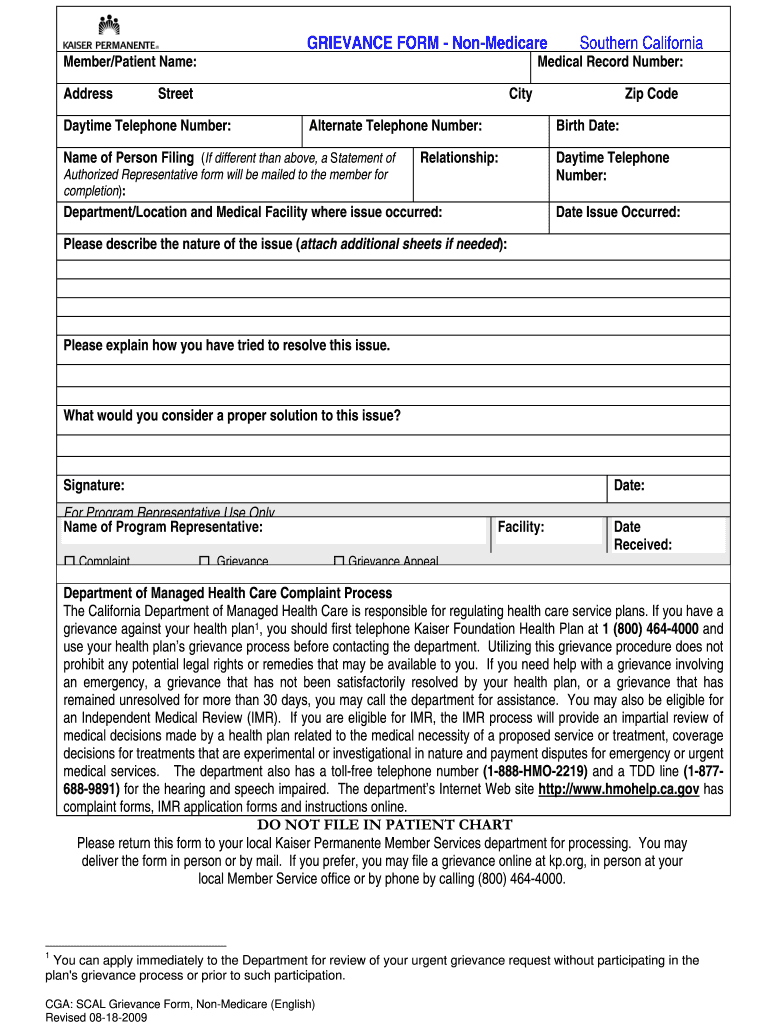
Kaiser Permanente Grievance Form Southern California 2020 2022 Fill And Sign Printable Template Online Us Legal Forms
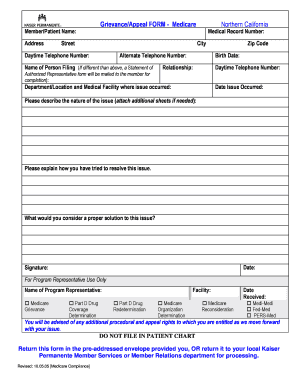
Fillable Online Info Kaiserpermanente Medicare Grievance Form Info Kaiserpermanente Fax Email Print Pdffiller

Editable 20 Kaiser Permanente Doctors Sick Note Kaiser Doctors Note Template Excel In 2022 Doctors Note Template Doctors Note Notes Template
2
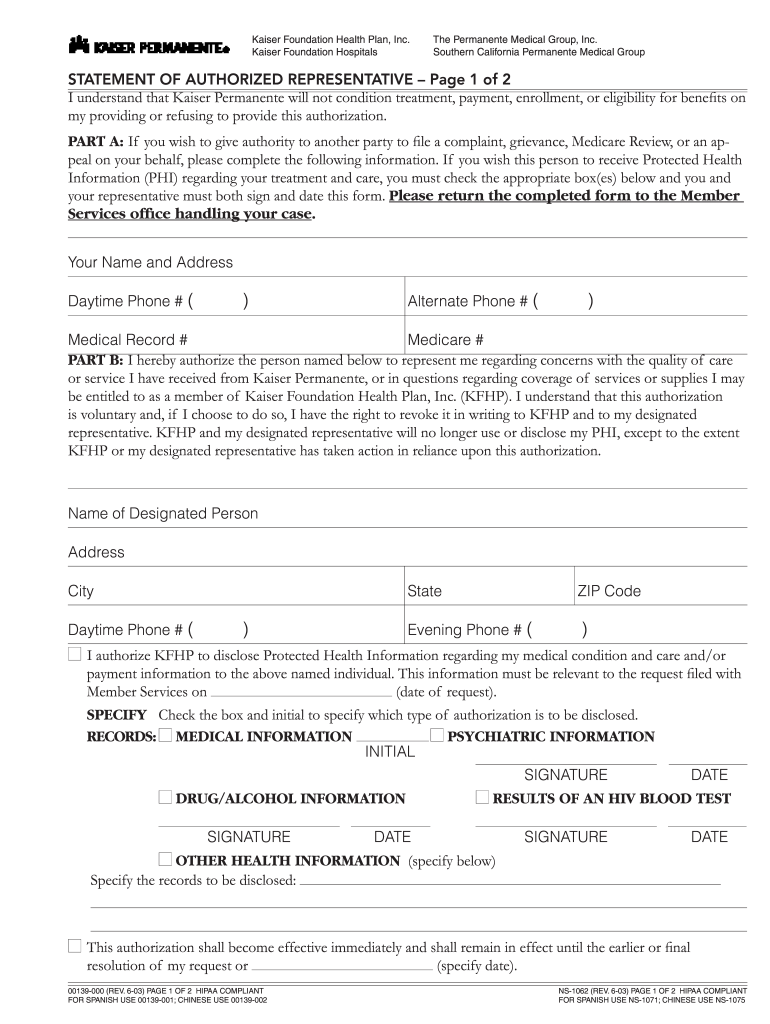
Kaiser Permanente Ns 1062 2003 2022 Fill And Sign Printable Template Online Us Legal Forms

Comparing Health Plan Types Kaiser Permanente Health Plan How To Plan Health Insurance Plans

Kaiser Permanente Jobs For Veterans G I Jobs
2
2
2
Application Kaiser Permanente California

Kaiser Permanente Rejecting Some Religious Exemptions To Employee Covid Vaccine Mandate Fox 5 San Diego
Kaiser Provider Appeal Form California Fill Online Printable Fillable Blank Pdffiller
Group Election Request Form Northern California Or Southern California Region